Article Text

Statistics from Altmetric.com
Worldwide, under-fives mortality has halved since 1990 from 93 to 41 deaths per 1000 live births in 2016. However, progress has been very uneven. Child mortality is still highest in Africa (76 per 1000 live births) (figure 1) and neonatal mortality has declined at a slower rate so is now approaching 50% of all under-fives mortality.1 Research and programmatic efforts are focussed on reducing child mortality in the highest burden areas. An intriguing and controversial idea to reduce mortality has arisen from mass antimicrobial distribution programmes for the prevention of blindness caused by trachoma.

Reproduced from https://www.unicef.org/publications/files/Child_Mortality_Report_2017.pdf,1 with permission.
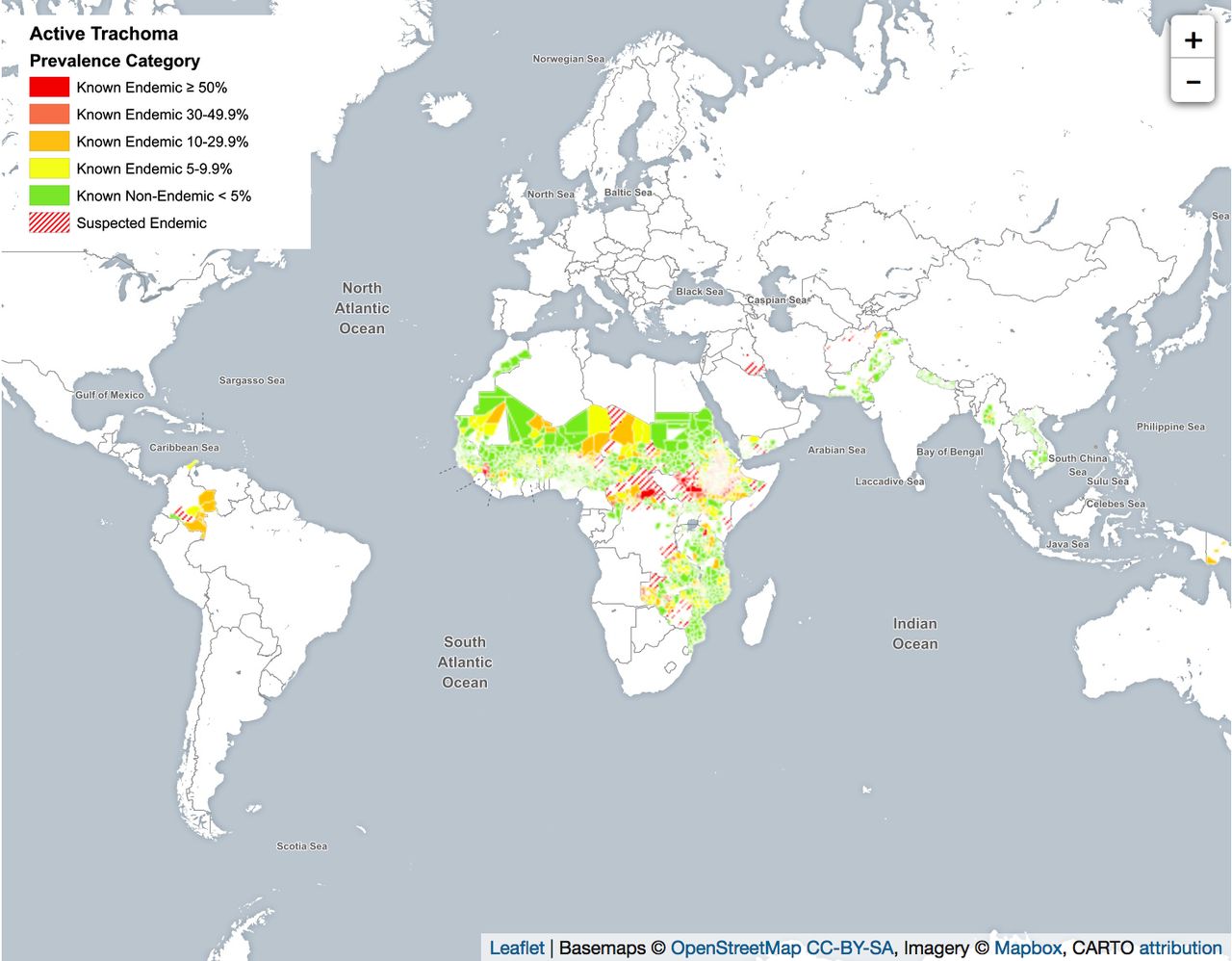
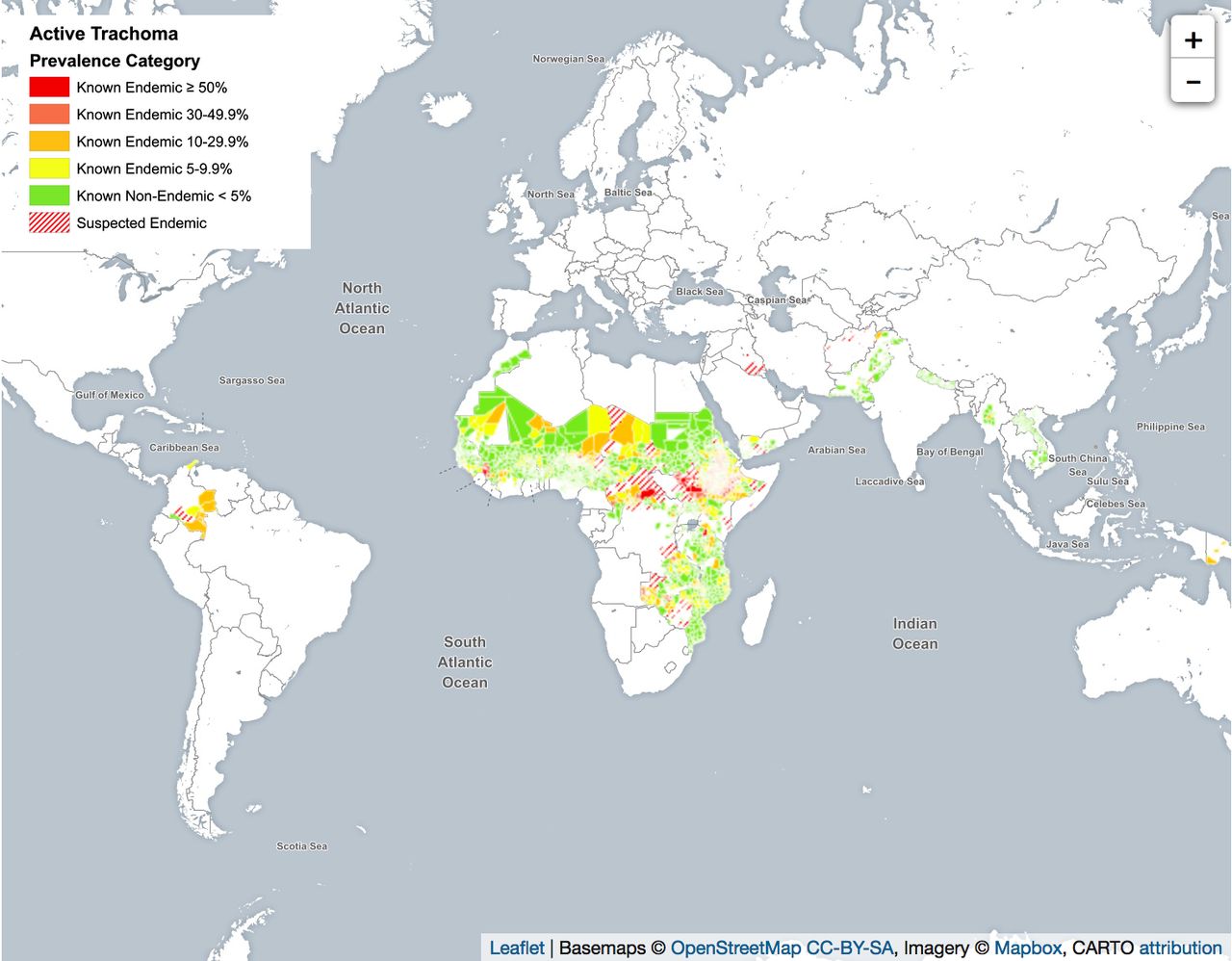
Trachoma has a predilection for the poorest, most remote communities with low levels of hygiene. Chlamydia trachomatis is spread by direct contact with fluid from an infected person’s eyes or nose, or indirect contact with these fluids via clothing or flies. It is endemic across Africa from South Sudan and Ethiopia (which have the highest prevalence of trachoma worldwide) across the dry Sahelian belt to Guinea and Mauritania in West Africa, and down through East Africa as far South as Malawi, Zambia and Mozambique (figure 2). The WHO estimates that there are 18 million cases of active trachoma in Africa, representing 85% of all cases worldwide. This large trachoma-endemic area in Africa encompasses 15 of the 20 countries with the highest reported under-fives mortality rates worldwide (79–133 per 1000 live births in 2016). Trachoma also occurs in areas of Asia, Central and South America, Australia and the Middle East. To eliminate trachoma, a four-pronged strategy of Surgery, mass Antimicrobial distribution, Facial cleanliness interventions and Environmental improvement (the SAFE strategy) has been adopted. To date, hundreds of millions of doses of azithromycin have been given for trachoma control.
{kind=link}
{kind=link}
Reproduced from http://www.trachomaatlas.org/global-trachoma-atlas, with permission. Prevalence maps were developed by the International Trachoma Initiative and present the prevalence of TF in children aged 1-9 years by district. Information is based on the most recent population-based surveys reported by program managers. Cartographic boundaries are meant to reflect program activity and are not necessarily true political boundaries.
In 2009, a striking finding was published from a cluster-randomised trial of mass azithromycin distribution in Ethiopia.2 Communities were randomised to annual or biannual azithromycin for all residents, or quarterly azithromycin for children only or treatment delayed for 1 year. The mortality rate among children aged 1–9 years in treated communities was half that of untreated communities (OR 0.51; p=0.02). A subsequent case–control analysis by the same group reported an OR of 0.31 (p=0.06) among children aged 1–5 years.3 The effect was unlikely to have arisen from control of trachoma because it is non-fatal.
Recently, the Mortality Reduction after Oral Azithromycin (MORDOR) trial was conducted in areas of very low trachoma endemicity in Malawi, Niger and Tanzania to test whether biannual mass single-dose azithromycin distribution during 2 years would reduce all-cause mortality.4 Overall, in ~1500 communities, ~190 000 children aged 1–59 months (or 12 months to 5 years) were involved. The community-based mortality rate was 13.5% (95% CI 6.7% to 19.8%, p<0.001) lower in azithromycin-treated communities than placebo-treated communities. The greatest reduction in mortality was in Niger (18%, p<0.001) where 72% of the more than 5000 deaths during the study occurred, with relatively little reduction in Malawi and Tanzania (6%, p=0.45% and 3%, p=0.77, respectively). Overall, infants aged 1–5 months had a 25% reduction in mortality. Using verbal autopsies after 250 deaths in each country, malaria was assigned as the leading cause of death (note that verbal autopsy may have low sensitivity and specificity for malaria mortality as febrile illnesses are difficult to distinguish5), followed by diarrhoea and pneumonia. Cause-specific efficacy could not be analysed.
The reduction in mortality is likely have been due to azithromycin’s previously demonstrated efficacy on acute respiratory infection, diarrhoea and malaria, potentially by influencing early or subpatent infection, carriage or transmission. A similar concept is successful in the intermittent preventive treatment of malaria in infancy or seasonal malaria chemoprevention (using older drugs that are not the current first-line treatment for malaria) in areas of moderate to high malaria transmission. Potential indirect effects could have also been due to impact on growth or the microbiome, but these await further analyses.
Communities in Niger had the highest overall mortality and thus a greater opportunity to demonstrate efficacy. However, communities in Niger are also generally more remote, poorer, with less access to healthcare or improved water and sanitation and more malnutrition. It may also be that there was less background antibiotic usage in the Niger communities, although this was not ascertained.
These results are exciting and of clear relevance to some of the most impoverished communities with the highest infant and child mortality rates worldwide. So, should this simple intervention be rolled out now in similar communities? The WHO have reserved judgement until more data are available because of uncertainty about the potential impact on antimicrobial resistance (AMR).
Only a few previous studies have examined resistance both before and after mass drug administration or have had a long enough duration of follow up.6 They suggest that macrolide resistant Streptococcus pneumoniae, Staphylococcus aureus and Escherichia coli carriage isolates are selected and expand rapidly following mass azithromycin administration. However, in communities with a low background prevalence of resistance, the increase is transient. Repeated dosing may cause a prolonged increase in resistance and require a prolonged drug-free period for resistance to decline. In areas with a high background rate of resistance an increase may not decline. There is unfortunately no information on invasive bacteria causing serious disease in this context. Further data on carriage of AMR are being collected in a subset of communities in each country in the MORDOR trial; all communities are being treated and followed in year 3 and then re-randomised in year 4. Information will be gathered on resistance in older untreated children in the MORDOR communities, and other trials are being rapidly initiated in West Africa. These data will be informative but will not answer deeply ethically challenging questions of how to balance demonstrated benefits for survival against less certain current and future risks associated with AMR.
What strategy will be recommended to reduce mortality (rather than trachoma control) is likely to be highly dependent on local rates of infant and child mortality, background rates of antibiotic resistance (which will align with access to treatment and care), whether a specific subset of communities can be targeted and the likely duration of any intervention. Targeting individual children most at risk may be feasible, but so far trials have been on effects in communities rather than individuals.
However, there is a bigger picture. The MORDOR trial provides strong evidence that in vulnerable resource-poor communities, a significant fraction of mortality is directly attributable to a lack of access to antibiotics. In a recent Lancet series, Ramanan Laxminarayan and colleagues estimated that currently more children may die from lack of access to antibiotics than from the effects of AMR and that improved access to antibiotics could reduce pneumonia-related deaths by 445 000 each year across 101 countries.7 At the same time, universal pneumococcal conjugate vaccine could substantially reduce antibiotic prescriptions. Ultimately, lives will be saved by improving access to preventive and diagnostic health services, improved nutrition, clean water and sanitation, bringing enormous other health and well-being benefits and helping children to achieve their potential without risks of AMR. While the short-term use of mass azithromycin distribution should be regarded as one potential tool to save lives in some specific settings, we should not take our eyes off the real prize. MORDOR is a highly informative study and a sharp reminder that not addressing basic needs results in considerable preventable infant and child deaths.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.